REPORTS
SGLT Inhibition for Type 1 Diabetes Management–How Far Have We Gone?
Presented by:Ele Ferrannini, MD, PhD
CNR (Consiglio Nazionale delle Ricerche), Institute of Clinical Physiology, Pisa, Italy
Paresh Dandona, MD
State University of New York at Buffalo, Buffalo, NY; USA
Juilo Rosenstock, MD
University of Texas Southwestern Medical Center, Dallas, TX; USA
John B. Buse, MD, PhD
University of North Carolina School of Medicine, Chapel Hill, NC; USA
David Cherney, MD, PhD
University of Toronto, Division of Nephrology, UHN, Toronto General Hospital Research Institute, Toronto, Canada
SGLT2 is expressed in the kidneys and may be overactive in patient with diabetes. In SGLT2-induced glycosuria, the creatinine clearance and fractional glucose excretion is higher in diabetes patients who are overweight or obese.1 In addition, the carbohydrate intake of men and women is affected based on body mass index (BMI) as is the lipid oxidation during fasting and mealtimes.2,3 The implementation of SGLT2 inhibitors raises endogenous glucose production, lowers tissue glucose disposal, and stimulates lipolysis and ketogenesis.3
This SGLT2-induced glycosuria leads to a shift in oxidative metabolism from carbohydrates to lipids. The resulting carbohydrate deficit is more apparent in lean individuals than in obese individuals. The lower insulin/glucagon ratio and the increased delivery of free fatty acids stimulate hepatic ketogenesis. This metabolic setting may increase the risk of ketoacidosis if there is an insulin or carbohydrate deficit.
The DEPICT studies were two clinical trials with nearly identical designs with a different geographical footprint. The studies were designed to test the efficacy and safety of dapagliflozin as an add-on to insulin in type 1 diabetes. To be eligible for participation, patients had to have an HbA1c of 7.7% to 11.0%. Patient were randomized 1:1:1 to receive dapagliflozin 5 mg + insulin, 10 mg + insulin, or placebo + insulin. Patients were treated for 52 weeks after a ≤28 days screening period and 8-week lead-in period.
Both dapagliflozin groups in both trials effectively lowered HbA1c at week 24 and week 52 compared to placebo. There was a decrease in insulin dose for both dapagliflozin groups in the DEPICT-2 study that was maintained for 24 weeks compared to placebo. Insulin dose reductions were more pronounced in the DEPICT-1 study for 5 mg and 10 mg dapagliflozin groups, with a 7.7% reduction in the 5 mg dapagliflozin group and a 12.2% reduction in the 10 mg dapagliflozin group compared to 1.2% with placebo.
Both the DEPICT 1 and the DEPICT 2 studies demonstrated a statistically significant reduction in body weight with both dapagliflozin groups at week 24 (DEPICT-1 and 2) and week 52 (DEPICT-1), compared to placebo. The proportion of patients with a HbA1c reduction ≥0.5% without severe hypoglycemia episodes was higher in the 5 mg and 10 mg dapagliflozin groups compared to placebo at 24 weeks of the DEPICT-2 study (39.5%, 41.6%, 20.1%, respectively). Even greater HbA1c reductions without severe hypoglycemias were seen in the DEPICT-1 study at both the 24- and 52-week time point (24 weeks; 50%, 51%, 25% for 5 mg, 10 mg and placebo, respectively; 52 weeks; 40.2%, 42.1%, 23.7% for 5 mg, 10 mg and placebo, respectively). Continuous glucose monitoring (CGM) endpoints at week 24 showed improvements in mean 24-h interstitial glucose levels for both dapagliflozin groups, compared to placebo, in both DEPICT studies.
The most frequent adverse events were related to genital and urinary tract infections which occurred more frequently in both of the dapagliflozin groups compared to placebo. Diabetic ketoacidosis (DKA) was also more prevalent in patients in both the dapagliflozin groups compared to placebo, in both the DEPICT studies.
The DEPICT studies demonstrate that dapagliflozin treatment in type 1 diabetes was well tolerated over 52 weeks, with improvements in glycemic control and weight, reductions in insulin dose and glycemic variability, and no increase in hypoglycemia, but with more DKA events.
The EASE-1 phase 2 study was a small randomized, double-blind, placebo-controlled, 4-week trial in two European sites.4 The goal of the trial was to investigate the pharmacodynamics, efficacy, and safety of empagliflozin as an adjunct to insulin in patients with type 1 diabetes.4 A total of three empagliflozin daily doses were used: 2.5 mg, 10 mg, and 25 mg. In the 28-day study, empagliflozin, when used as an adjunct to insulin, was effective in increasing urinary glucose excretion, improving HbA1c, and reducing weight with lower insulin doses compared to placebo.4
The EASE-2 trial was a 52-week trial investigating empagliflozin 10 mg and 25 mg compared with placebo, while the EASE-3 trial was a 26-week trial using empagliflozin 2.5 mg, 10 mg, and 25 mg compared with placebo. To be included in either of the trials, patients had to have type 1 diabetes for a least 12 months (C-peptide <0.7 ng/mL) and be on multiple daily injections (MDI) (≥12 months) or continuous subcutaneous insulin infusion (CSII) (≥5 months) prior to screening. HbA1c range was ≥7.5% to ≤10.0%. The primary endpoint was change in HbA1c from baseline, with rates of symptomatic confirmed hypoglycemia, as well as others (body weight, total daily insulin dose, and blood pressure changes), as the secondary endpoints.
The three tested doses of empagliflozin induced HbA1c reductions, weight loss, and no increases in symptomatic or severe hypoglycemia compared to placebo. The 10 mg and 25 mg empagliflozin groups confirmed higher rates of DKA. Results are not publicly available but will be presented at the EASD in October 2018.
Sotagliflozin is a dual inhibitor of both SGLT1 and SGLT2. As a review, SGLT1 is expressed in the intestine and is the major transport molecule involved in the absorption of glucose and galactose. It also plays a minor part in the kidney in regards to glucose absorption. When SGLT2 is blocked in the kidney, it results in increased urinary glucose excretion.5,6 The use of both an SGLT1 and SGLT2 inhibitor delays the post-meal glucose levels compared to SGLT2 inhibitors or no treatment.5,6
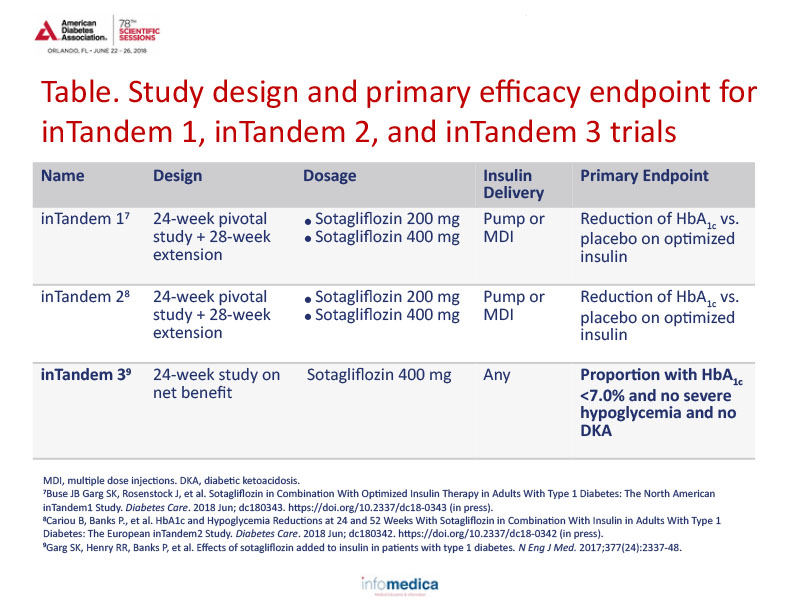
Sotagliflozin was studied in three tandem clinical trials, labeled inTandem 1, inTandem 2, and inTandem 3. See Table to review the study design and primary efficacy endpoint for each trial.
In a pooled analysis of sotagliflozin inTandem 1 and 2, both the 200 mg and 400 mg sotagliflozin groups statistically lowered the HbA1c from baseline as well as absolute body weight compared to placebo at 24 and 52 weeks.10,11 Sotagliflozin demonstrated statistical significant efficacy at 52 weeks in reducing total insulin dose (200 mg and 400 mg), basal insulin dose (200 mg and 400 mg) and bolus insulin dose (400 mg only) when reviewing pooled inTandem 1 & 2 data compared to placebo.10
A subset of inTandem 1 & 2 patient data was explored with CGM for the time spent in glycemic ranges for sotagliflozin vs placebo groups. At 24 weeks, the sotagliflozin 200 mg increased the time in glycemic range from 12 hours and 32 minutes at baseline to 13 hours and 52 minutes.12 The sotagliflozin 400 mg group increased the time in glycemic range from 12 hours and 10 minutes at baseline to 15 hours and 25 minutes.12 There were more adjudicated cases of DKA in the treated groups compared to placebo.10,11 Documented cases of hypoglycemia were less frequent with sotagliflozin.
In the inTandem 3 study, the net clinical benefit at 24 weeks (proportion of patients with HbA1c <7.0%, no severe hypoglycemia, and no DKA) was statistically higher in the sotagliflozin group compared to placebo (28.6% vs 15.2%, respectively) as was the HbA1c reduction from baseline.9 In addition, in the inTandem 3 trial, more patients achieved an HbA1c of <7% and related benefit-risk endpoint in sotagliflozin vs insulin alone. There were more adjudicated cases of DKA in the sotagliflozin treated groups compared to placebo.13 Documented cases of hypoglycemia were less frequent with sotagliflozin also in the InTandem3.
Limited therapies are available for cardiorenal protection in patients with type 1 diabetes. This is an unmet need as many of these patients have increased rates of CVD, CHF, and DKD. To date, there is no evidence that supports the use of novel antidiabetic therapies for type 2 diabetes in end-organ protection.
Diabetes causes glomerular hypertension which can be reduced with the use of SGLT2 inhibitors.14 Preliminary animal studies have demonstrated an effect on afferent arteriole vasoconstriction with SGLT2i which is likely affected by natriuresis.15 When type 1 diabetes patients were treated with empagliflozin, a reduction in renal blood flow and an increase in renal vascular resistance were observed which was consistent with the afferent arteriole vasoconstriction seen in animal studies.14 Renal hypoxia is also a concern in diabetes patients. In an animal study exploring renal cortex oxygen, animals with type 1 diabetes had lower levels of oxygen compared to healthy controls and phlorizin-treated animals.16
Inflammatory biomarkers have been demonstrated in patients with type 1 diabetes and a reduction of those markers has been seen with SGLT2i use. However, there have not been any studies reviewing inflammatory markers in type 1 diabetes.17
There are a number of overlapping benefits that have been demonstrated, in human or animal trials, that appear to cross both type 1 and type 2 diabetes. These include:
- ↓Hyperglycemia, low risk hypoglycemia
- ↓Body weight
- ↓Insulin requirements
- ↓Blood pressure
- Hemoconcentration
- ↓Renal hyperfiltration
- ↓Plasma uric acid
Key messages
- SGLT2-induced glycosuria leads to a shift in oxidative metabolism from carbohydrate to lipids.
- There is an additional risk of DKA under circumstances of insulin and/or carbohydrate deficit.
- Dapagliflozin has been the first selective SGLT2 inhibitor as add-on to insulin in type 1 diabetes that demonstrated reductions in HbA1c, total daily insulin dose, and body weight over 52 weeks.
- Adjunctive therapies to insulin are still an unmet need in type 1 diabetes.
- There is an increased risk of serious DKA when using SGLT inhibitors.
- Sotagliflozin is a dual SGLT1/SGLT2 inhibitor that simultaneously increases urinary glucose excretion and slows intestinal glucose absorption.
- Sotagliflozin, in combination with insulin in type 1 diabetes, doubled the proportion of patients achieving HbA1c below 7.0% with no severe hypoglycemia, but with more DKA events, compared to insulin alone at 24 and 52 weeks.
- Sotagliflozin was well tolerated in adults with type 1 diabetes when added to insulin.
- Cardiorenal outcome trials are urgently needed in type 1 diabetes.
REFERENCES
Present disclosures:
Ele Ferrannini: the presenter has disclosed that he has been a board member, advisory panel member, and consultant to Boehringer-Ingelheim/Eli Lilly, Sanofi. He has received research report from Boehringer-Ingelheim, Eli Lilly, and Astra Zeneca and has been on the speaker’s bureau for Astra Zeneca, Takeda, Novo Nordisk, Sanofi, Tanabe/Mitsubishi, and Boehringer Ingelheim.
Paresh Dandona: this presenter has no disclosures to report.
Juilo Rosenstock: the presenter has disclosed that he has received research support from Merck, Pfizer, Sanofi, Novo Nordisk, Bristol-Myers Squibb, Eli Lilly, GlaxoSmithKline, Astra Zeneca, Lexicon, Janssen, Intarcia, Genentech, and Boehringer Ingelheim. He has also been involved in advisory boards or received consulting honorarium from Novo Nordisk, Sanofi, Eli Lilly, Intarcia, Janssen, and Boehringer Ingelheim.
John B. Buse: the presenter has disclosed that he has received research support from Astra Zeneca, Boehringer Ingelheim, Johnson & Johnson, Lexicon, Novo Nordisk, Sanofi, Theracos, and vTv Therapeutics. He has consulted for Adocia, Astra Zeneca, Dexcom, Elcelyx Therapeutics, Eli Lilly, Intarcia Therapeutics, Lexicon, Metavention, NovaTarg, Novo Nordisk, Sanofi, Senseonics, and vTv Therapeutics. The presenter also has stock options for Mellitus Health and PhaseBio Pharmaceuticals.
David Cherney: the presenter has disclosed that he has received consulting and honoraria from Boehringer Ingelheim, Lilly, Janssen, Merck, AstraZeneca, Mitsubishi-Tanabe, and Sanofi. He was also involved in the following trials; CREDENCE, TRANSLATE, BETWEEN, DIAMOND, DAPA-CKD, SCORED, EMPA-CKD, INDORSE, ERADICATE-HF.
Written by: Debbie Anderson, PhD
Reviewed by: Marco Gallo, MD